Nose Surgery Rhinoplasty5 Nostril Narrowing
Nose Anatomy - Alae (Nostrils)








")


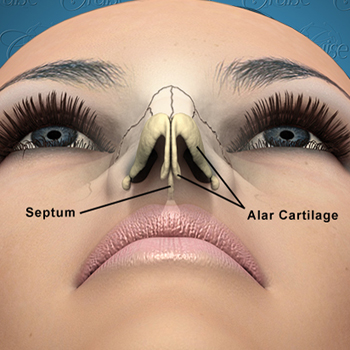
Nasal Alae
The alae form the sidewalls of the nostrils. They are responsible for keeping the nostrils open and to help give support to the tip.

The two alae
The alae play a significant part in maintaining the airway. Significant airway problems can occur If they are narrowed or they collapse with inspiration. Correction of these problems often involve strengthening the alar cartilages with a cartilage graft.
When looked at from below, the alae and tip should ideally form an equilateral triangle (all three sides of the triangle being the same).

Ideal nose as viewed from below
Outlined below is a view with the skin removed showing how the alar cartilages support the nostrils.
The three most common cosmetic complaints regarding the alae are:
- Wide, Flaring Alae
- Notched Alae
- Asymmetric/Deformed Alae
Let's take a look at each of these. Hopefully, this will allow you to better understand what is going on with your alae and all of your nose anatomy. With this in mind, you will be better able to identify to your plastic surgeon exactly what you want to achieve.
Wide Alae
If the alae flare too much this will give the nose a wide appearance.
Wide Alae Visualized

Wide, flared alae

Alar exicion. Area in read is removed to correct wide alae.
Treatment of Wide Alae
Correction of a wide alae is typically done by excising a portion of the alae just as it connects with the face. This predictably leaves a scar that is not recognizable.
Alar excision must be done precisely else the nose can look unnatural or leave a visible scar. Alar excision is modified depending on the anatomy of the nose. It takes an experienced rhinoplasty surgeon to know exactly how this excision is performed.
Caution: Not all wide alae can be reduced even though my patients may really what them to be. If the nasal vault is wide then the alae must be wide. Otherwise, you will create the deformity known as the “Bowling Pin” deformity.
Carefully look below. On the left you will see a wide alae that is correctable by an alar excision. This is because the alae abruptly flare out compared to the middle portion of the nose.
Compare this to the image below on the right. This wide alae is not correctable. This is because the alae does not flare out abruptly. This alae flares out gradually starting farther up the nose.
Alae Correction

Alae correctable with alar excision

Alae not correctable with alar excision
Why can't the flared alae on the upper right be corrected? The reason is: if the alae is made as narrow, or worse yet, even narrower than the middle part of the nose it will look unnatural and “operated on.”
If the nose on the right does have an alae resection, it will create a "Bowling Pin" deformity as shown below.

Bowling Pin deformity
Notice how the alae curve inward at the bottom. The key to rhinoplasty is to make the nose look like it was never operated on. The bowling pin deformity immediately alerts everyone that something was done.
Alar Notching
Notching of the alae occurs when the alae arches upwards, exposing the inside of the nose. It can cause the nose to have a "snarl" appearance even when the nose is completely relaxed.

Alar notching
Similar to a hanging columella, notching of the alae may not be a problem unless it is severe. Notching is common in patients who have had a rhinoplasty. This is because when the tip was made smaller, the alae retracted upward.
This is why it is important for the surgeon to take steps during the rhinoplasty to make sure notching does not occur.
Treatment of Alar Notching
Typically, notching is treated by strengthening the lateral crura. The increased strength and size of the lateral crura will push the notching downward. Severe cases require more aggressive techniques that are beyond the scope of this outline.
Asymmetric / Deformed Alae

Asymmetric alae
As you can image, there are many variations on what could cause the alar cartilages to be asymmetric. The image above depicts a deformed, weak alar cartilage on the patient's left. Correction often requires that the alar cartilage be reinforced or sometimes completely replaced with a cartilage graft.
This is where surgeon's experience is paramount. Even with the most experienced surgeons, complete symmetry will not be obtained. The reason for this is that, in these cases the soft tissues are also deformed. So, even when the underlying cartilage support is corrected, the overlying skin and soft tissue will remain asymmetric. This often, cannot be corrected.
