
Breast Augmentation FAQs
Breast Augmentation FAQ's
Questions
- Word of mouth. If you know someone with a good result and a overall good experience than this plastic surgeon should be seriously considered.
- It is important to know how many breast augmentations does the plastic surgeon perform in a month. My recommendation is that the surgeon should do at least 4 a month. This shows that he or she has the recent experience necessary. This can be verified by asking the patient coordinator to show you the surgeon's schedule for the last month.
- How comfortable do you feel with the plastic surgeon and the office in general. This can not be emphasized enough.You must be able to place a great deal of trust in their hands. Does the surgeon answer your questions? Does the patient coordinator genuinely help you through the process?
- How comfortable are you with implant sizing process. Remember the number one reason for re operation after breast augmentation is for change of implant size. While dissatisfaction with implant size can not be eliminated it can be markedly reduced. This requires proper interviewing by the surgeon and proper bra sizing by the patient coordinator. You should be able to leave your consultation with confidence that the time was taken to determine what size is best for you. If you do not feel this than you should look elsewhere.
- Ask to see before and after pictures performed by the surgeon and not by some other surgeon. This makes sense. The surgeon should be able to provide plenty of examples of his or her work. If he/she says most patients don't authorize their photos to be used, this could be a red flag.
- Is he or she board certified? Be careful to make sure he or she is board certified by the American Board of Plastic Surgery and not some other board. Must be certified in the field of plastic surgery.
- Make sure the plastic surgeon uses a board certified anesthesiologist to administer anesthesia. Remember, the most important thing is safety.
Eighteen is the minimum age I recommended, as well as it being the policy of the American Society of Plastic Surgeons. The FDA recommends a woman is 18 yrs or older for saline and 22 yrs or older for silicone. The reasons I recommend a minimum age of 18 are as follows:
- Teens and their parents may not fully realize the risks associated with implants.
- A teen's body often has not yet fully developed.
- A teen may not be psychologically ready to handle the outcome or potential complications.
This is one of the most commonly asked questions I hear at my practice. The answer is not simple. There are many variables but we will try to make it as clear as possible.
In general, if the nipple is above the Infra-Mammary Fold (the fold below the breast tissue) then a breast lift is not usually necessary. If the nipple is more than 1 centimeter (about one-half inch) below the Infra-Mammary Fold (IMF) then a breast lift is most likely required.
What about the nipple that at the level of the IMF? With this situation, the need for a breast lift depends on two things:
How big will the implant be. It stands to reason that a bigger implant will create more of a lift.
What bothers you more; low nipples or scars around the areola. The scars are not very noticeable but they are still scars.
Remember, if you elect not to have a breast lift, you can always have it done later on.
Tubular breasts are also called constricted breasts. Tubular breasts have many variations, the most common ones include:
- High and tight folds
- Very narrow base
- Protruding nipples
- Herniation of the breast tissue through the areola
- Abnormally broad areolas
Augmentation alone many times may correct tubular breasts. If there is a significant amount of ptosis, or the areolas are very large, a Benelli or anchor lift may be necessary to correct the malformation.

Before Breast Augmentation (above)
3 months after breast augmentation with 450cc silicone breast implants, through areola incision, above the muscle. Notice the tension on the skin on the lower portion of the breasts.

6 months after the surgery the implants took over the shape of the breasts. The bottom of the breasts is no longer tense like it was at 3 months.

Before Side View

After breast augmentation the nipple is no longer protruding and the base of the breast is naturally round.
Tubular breasts take longer to achieve the roundness and fullness than average breasts. With time, however, they achieve nice and round shape. Silicone may be a better option for correction of constricted breasts, especially in patients with very little breast tissue. The implant creates the breast shape.
Size, Shape, Implant Placement
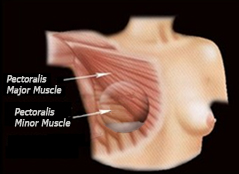
Deep to the breast tissue is the pectoralis major muscle. Breast implants can be placed either on top of this muscle or underneath it. See pictures below.
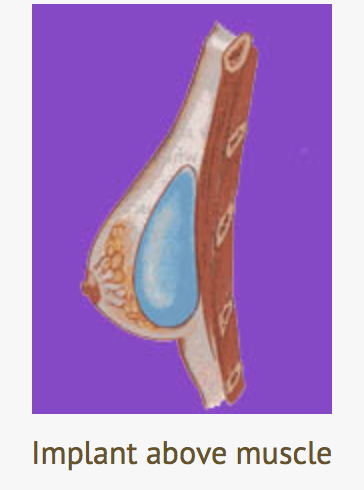

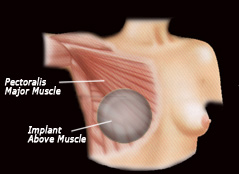
When the implant is placed on top of the muscle it is closer to the skin and therefore may be more easily felt and appear more rounded superiorly in patients with little breast tissue. If a patient is a B cup or greater, implant visibility is not a problem. Therefore, the implant can be placed either under or above the muscle with excellent aesthetic results. Implant placement below the muscle, however, has a slightly lower risk of capsular contracture.
Implant Above Muscle
Of note, even when an implant is placed under the muscle the bottom and lateral part of the implant are not completely covered by the muscle.
Depiction of how lateral/inferior 1/3 of implant is not covered by muscle even if placed submuscularly.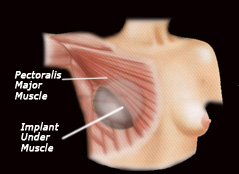
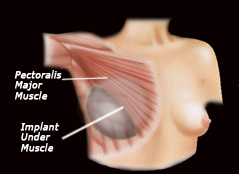
The amount of uncovered implant goes up considerably when larger implants are placed. This is why rippling may occur along the lateral and inferior aspect of the breast especially with larger implants.
Notice that as the implant becomes larger,less of it is covered by the pectoralis major muscle
Which is better? Above the muscle or below?
The answer is not completely straight forward and depends on the amount of the amount of natural breast tissue and amount of breast sag, if any, that the patient has. Outlined below are four possibilities:
- Patient with little breast tissue and no sag. In these patients, implant placement above the muscle would likely create an "implant look". The superior part of the breast would be unnaturally round. In addition, because there is little natural breast tissue to cover the implant rippling would be more likely. For these reasons, implant placement below the muscle is usually the best choice.
- Patients with moderate amount of breast tissue and no breast sag. These patients have a choice. If they desire a large implant than below the muscle is probably best. If they go with a moderate implant or smaller then implant placement above or below the muscle are both acceptable. One caveat, in athletes or bodybuilders who need full use of their pectoralis major muscle, placement above the muscle may be a better choice as the muscle is not altered.
- Patients with small amount of breast tissue and breast sag.In these patients, it is usually best to put the implant under the muscle and perform a breast lift. If silicone implants are use than above muscle placement is also acceptable as silicone has a more natural appearance and is less likely to show rippling.
- Patients with moderate or large amount of breast tissue and also breast sag.These patients are best served when the implant is placed above the muscle in conjunction with a breast lift. This is so that the natural breast tissue and the implant are allowed to integrate into one. This provides a more natural appearance and lessens the chance of "double bubble."
Advantages of placement under the muscle:
- Lower risk of rippling. Once again, if you have large implants the inferior and lateral portion of the implant is not under the muscle, therefore is more likely to have rippling regardless of placement. If you have a moderate amount of natural tissue then rippling is unlikely regardless of placement.
- Lower risk of capsular contracture. It is thought that the constant flexing of the muscle acts like a massage to the capsule, therefore it is kept softer.
- There is less of an "implant look."This mostly applies to the superior aspect of the breast when the patient has little natural breast tissue. The muscle softens the upper pole of the implant. This causes the implant to have more of a sloped look and less of a rounded, implant look. When a patient is a B cup or larger this becomes less relevant.
- Mammograms are slightly more accurate. Because the breast tissue is separated from the implant by the muscle the breast tissue is easier to see on mammography.
Advantages of implant placement above the muscle:
- In women with well developed pectoralis major muscles such as body builders, it is possible that the muscle will move the implant with shoulder movement. This can be very annoying. In body builders I recommend silicone implants over the muscle.
- Allows for more natural appearance in patients who have a significant amount of natural breast tissue. This is because the implant and the breast tissue are not separated and are allowed to become one.
- Allows for a more natural appearance in patients with breast sag. In these patients the placement of the implant below the muscle will separate the breast tissue from the implant and may create a double bubble appearance. This is caused because the implant is held up higher on the chest wall by the muscle and the natural breast tissue sags lowers creating an unnatural separation.
- Less discomfort during recovery. Since the muscle is not stretched there is less of postoperative pain.
The short answer is "No." Over the years I have developed a technique where I place the lateral aspect of the implant under the Serratus Anterior muscle. This effectively covers the part of the implant that is most likely to show rippling via the conventional "under the muscle" technique. By placing it under both the pectoralis major and serratus anterior almost all of the implant is covered by muscle.
Implant under both Pectoralis Major and Serratus Anterior Muscles. Not all women have a developed enough Serratus Anterior but, if present, it does provide additional coverage.
Of note, a small percentage of women have a poorly developed serratus anterior muscle making total muscle coverage impossible. In this situation the implant is still covered by the pectoralis major muscle. With large implants, the inferior part of the implant remains uncovered.
There are several ways to determine implant size. One way is for the surgeon to place different sizers during the operation. The other way is to do bra sizing during your consultation. I believe that it is critical to determine implant size prior to going into the operation. I do not believe in having the surgeon put trial sizers on during the operation because on the surgery table the breasts do not look like they normally do. Furthermore, this technique does not take into account how the breasts adapt over time. Finally, this method relies on the surgeon deciding on what is best for the patient. In my opinion, it is important to try on trial bras during your consultation, form fit it and then look at yourself in the mirror. Not all plastic surgeons do this, therefore, you can improvise by filling zip-lock bags with appropriate amount of rice and place them in your bra to get an idea. As you can imagine, this is not as accurate.
It is very helpful to bring in a picture of someone with a similar body type to you who has breasts that you would like. This helps immensely to demonstrate size, shape, and implant position. Do not be embarrassed! Remember, dissatisfaction with implant size is the number one reason why implanted women have to exchange their implants.
There is a number of factors influencing the size you will choose. And it should be always you who chooses the implant size. You might take into consideration opinions of your spouses, friends, etc. but you will be the one who carries them ultimately. This is why it is very important that you feel comfortable with the size you choose. Our patient coordinator will help you figure the size and match it with your body size, look for proportion and symmetry.
The three common incisions are:
- Infra-mammary (in the breast fold)

- Peri-areolar (under the nipple where the dark skin meets the lighter skin)
- Trans-axillary (armpit)
The best incision is the one that your plastic surgeon does most often and feels most comfortable with. This can not be overemphasized. It is important to not change a surgeons routine. If he or she does not normally do breast augmentation using the incision you demand, go to another plastic surgeon who does. I have found that the peri-areolar incision allows for the least visible scar and also provides the most accurate implant placement.
Each incision has its pros and cons. All 3 incisions can provide excellent results.
- Infra-mammary.The incision within the fold at the bottom can provide excellent results but the scar can be more noticeable than the other two incisions depending on how well you heal. This approach may be necessary if you decide on large silicone implants that can not be inserted via the other two incision sites.
- Peri-areolar. The incision along the margin of the areola allows for very accurate implant placement. The scar becomes almost imperceptible within 2 months in most women.
- Trans-axillary. The axillary incision can also provide a great result but the tradeoff is that implant positioning is not as easily adjusted from this distant site. This topic is discussed more in Joseph T Cruise, MD's Philosophy section.
- Naval incision. Not as common as the other three.Some plastic surgeons use this incision but the results, when compared to the standard incisions, are not as predictable. This is because it is impossible to visualize the pocket where the implant will be placed. For this reason Joseph T Cruise, MD, and most plastic surgeons, no longer perform breast augmentation via this approach. This is not to say that this incision cannot produce good results. It is just that the results are less predictable and Joseph T Cruise, MD only performs procedures with predictable results.
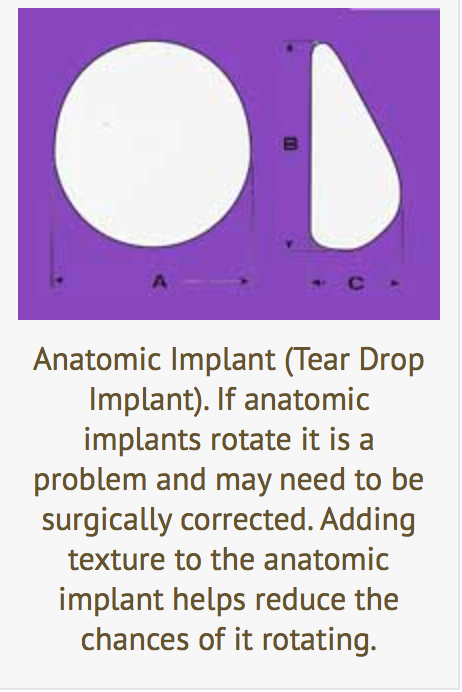
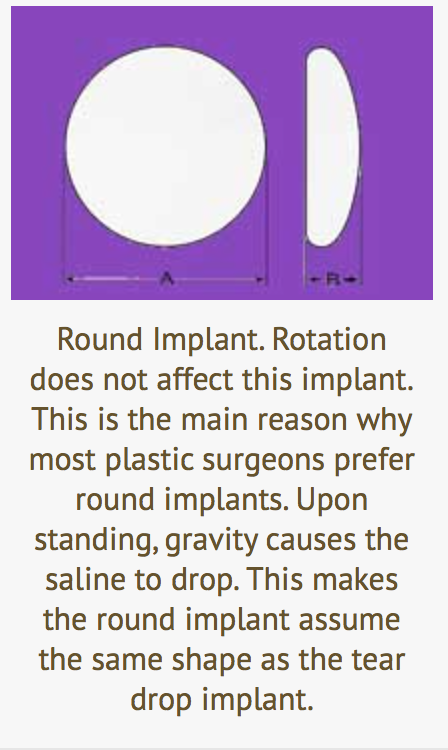
Most plastic surgeons use round, saline implants. Round has become the favorite because there is no way for it to become mal positioned because of rotation. If tear drop shaped implants rotate they may need to be surgically repositioned. The fact is, when you are standing round implants assume a tear drop shape anyway because gravity naturally causes the saline to descend. This makes the implant bigger at the bottom of the breast and smaller near the top.
What are textured implants?
n the 1970's capsular contracture was a much bigger problem than it is today. It was found that by adding texture to the shell of the implant the capsule that formed around the implant was much thinner and softer. It was found that the texture caused tissue ingrowth which broke up the collagen that formed around the shell. Textured implants still have a slightly lower rate of capsular contracture today but the advantage is not as significant because the smooth shells have been improved dramatically.
Who should get textured implants?
There are two types of women who can benefit from textured implants.
Women who have developed capsular contracture with smooth or silicone implants and need to do everything they can to prevent it from recurring. They should have their previous implants removed, the capsule removed and textured saline implants placed under the muscle. This is the best chance of preventing recurrence of capsular contracture.
Women who desire anatomic implants a.k.a. tear drop implants. If anatomic implants turn within their pockets they will not be positioned correctly because they are not round. When round implants turn it does not matter because round implants are in proper orientation no matter how they rotate. This is not true for anatomic implants. When they turn they are no longer oriented properly. This can be a big problem. Textured implants are less likely to rotate.
Silicone, Gummy Bear & Saline Implants
- Silicone breast implants are made with a silicone outer shell and come pre-filled with silicone gel. The gel feels closer to natural breast tissue than saline.
- Saline breast implants are made with an outer silicone shell that come empty and are filled with sterile salt water once implanted into the body.
- Form-stable implants are often referred to as gummy bear breast implants, because if the implant shell breaks, they maintain their shape due to the thicker cohesive gel inside. They are made with a silicone outer shell and come pre-filled with thick cohesive silicone gel on the inside. The tend to be firmer than regular silicone implants.
- The Ideal Implant is a hybrid saline implant that is similar in look and feel to a silicone implant, but has the safety of saline. The structured Ideal Implant has an inner shell around the inner chamber, which holds the inner saline filler, and an outer shell around the outer chamber, which holds the outer saline filler. Between these shells are one to three baffle shells. This internal structure controls movement of the saline and gives the Ideal Implant its natural feel. It contains no silicone gel or new materials.
At the time there were concerns about an increased risk of auto-immune and connective tissue diseases from the silicone.
Over the past 14 years numerous studies have shown silicone to be safe. There appears to be no increased risk of disease. In addition, similar studies in Europe where the implants were never taken off the market show it to be safe as well. With all this information, the FDA gave silicone breast implants its approval. Studies will continue.
Saline has several advantages over silicone:
- Sixty per cent of the human body is made of saline. Therefore, if there is a rupture the saline just gets flushed out of the body. With silicone, the gel remains and is much harder to remove it completely.
- The incision to put silicone implants in is a little longer than that of saline. This is because saline implants go into the breast empty and then are inflated, silicone implants, on the other hand, go into the body already filled.
- Cost. Silicone implants cost more.
Silicone has two significant advantages:
- It feels more like breast tissue. The gel-like feel is more natural than the fluid-like feel of saline.
- Silicone gel is less likely to ripple than saline.
No, there doesn't appear to be any increased risk with either silicone or saline implants.
Neither silicone or saline implants are meant to last a life time. Anyone considering breast augmentation should anticipate the need to have at least one more surgery on their breast. This may be because of implant exchange, change in size, breast lift, etc. The main difference is that saline implants do NOT HAVE to be replaced unless there is a problem. Silicone implants, on the other hand, should be replaced every 10-15 years even if there is no problem.
The reason is because a small rupture in a silicone implant may not change the breast shape. The silicone may get out of the implant shell but it will remain in the capsule that forms around the implant. This exposes the body directly to the gel. This has not been shown to be a problem but implant removal/exchange is still highly suggested.
There is no "ideal" time. Simply, it is when the woman wants to have it done. Indications to exchange include the desire to have a more natural feel and if there is significant rippling with the current saline implant.
Possibly. Often women who are interested in breast lifting have given birth, lost weight or have aged. Commonly these will lead to loss of breast tissue in the upper part of the breasts. Silicone implants allow for this to be filled out with a more natural appearance than saline in these patients. Of further consideration is the fact that silicone gel is heavier than saline. Therefore large implants should be discouraged, or sagging may reoccur
Possible Complications
Capsular Contracture
When any foreign body is placed under tissue the human body defends itself by walling it off. This involves forming a capsule around the foreign body. The same is true for breast implants. All women form capsules around breast implants. The problem is, some people form very thick and hard capsules. In rare cases, this can distort the implant and even make it painful. It can occur months or even years after the implants have been placed. Capsular contracture can occur on one or both sides.

The chance of getting a capsular contracture that causes distortion after a breast augmentation is less than 4%. Saline implants are less likely to cause capsular contracture than silicone. Similarly, placement under the muscle is less likely to cause it than placement over the muscle. Finally, textured implants are less likely to harden than smooth implants. Theoretically, the best scenario to prevent capsular contracture is textured, saline implants placed under the muscle.
The most effective way to prevent capsular contracture is to perform daily massage of the implant. Massage is known to soften scar tissue. If you feel your breasts begin to become firm I recommend taking vitamin E daily.
In addition, I recommend taking Accolate twice a day for six months. Accolate is an asthma medication that blocks the production of leukotrienes which are known to contribute to inflammation and scar formation.
- Dissatisfaction with breast size. This is the most common complication of breast augmentation. More commonly, the implants are too small and the patient exchanges them for larger ones. Therefore, it is important that you feel comfortable during your consultation that your plastic surgeon and patient coordinator have meticulously gone over this with you. This requires bra sizing either with trial implants or, my favorite, bra sizers. This is important and can not be over emphasized.
- Wrinkling of saline implants. This is especially true with big saline implants over the muscle. Even under the muscle the lateral aspect of the implant is close to the skin and prone to wrinkling. I feel that if you plan to get a large implant it should be placed under both the serratus anterior and pectoralis major muscle. This, however, is not a common practice. Silicone implants are much less likely to ripple.
- Loss of nipple sensation <10%. This tends to improve over several months. Patients who choose larger implants are at higher risk of sensation loss.
- Asymmetry 7%. Once again bigger implants are more likely to be asymmetric because it is necessary to lower the infra-mammary fold. This make the procedure more complicated and increases the chance that both folds will not be lowered the same amount.
- Intense nipple sensation 5%. This tends to go away in several months. It is not uncommon for the nipples to be constantly erect.
- Capsular contracture 4%. I have an entire Capsular Contracture page devoted to the explanation, treatment, and more. If it happens it can be a bad problem that may not go away unless the implant is removed or re-operated on.
- Infection 2%.
You must understand that a breast implant is not designed to last a life time. It is likely at some point you will have your implants changed. This may be because you wish to change size or you need a lift. Remember, the number one reason for re-operation is dissatisfaction with implant size. It is critical that you feel that your plastic surgeon and patient coordinator know what you want. Other reasons include deflation or implant shifting. Many women in my office have had their implants for over 20 years and have not had a problem. If there is no problem, I tell them there is no reason to exchange them.
This depends on how big of an implant you have and the quality of your skin. If you have good quality skin, i.e. no stretch marks, and your implant is less than 400 cc's it is likely that your skin will recoil well and return close to where you were before the implants. If you are over 40 years of age or have stretch marks it is unlikely that your skin has the ability to recoil. This may result in loose skin or dimpling.
There is a small chance, < 3%, that you will lose sensation in your nipples. This is more likely with large silicone placed through a peri-areolar incision, The reason for this is that silicone implants are pre-filled. Saline implants, on the other hand, are placed in the pocket first and then inflated. This allows saline implants to be placed through a smaller incision with less trauma. If you are worried about nipple sensitivity and want to have silicone implants 450 cc's or larger than the infra-mammary incision may be best for you. Another consideration is the size of your areola. If you have very small areola it is harder to place silicone implants through the peri-areolar incision. Often after breast augmentation, women experience hyper-sensitivity. The nipples may become erect which can be uncomfortable. This goes away within a month or two.
Usually they do not. If, however, you go with large implants and have poor quality skin then it is possible that you will. Stretch marks are small scars within the dermis caused when the dermis is no longer capable of stretching. Massaging with Vitamin E twice a day may help to reduce the chances of developing stretch marks.
Breast implants require more X-rays during mammogram in order to see around the implant. For this reason, mammograms on women with implants often cost more. If you have a strong family history of breast cancer and/or significant fibrocystic disease you should be sure to discuss this during your consultation. It should be pointed out that breast augmentation does not increase the likelihood for breast cancer.
Both silicone and saline implants make mammogram screening slightly less effective. There is very little difference between silicone and saline. Both implants require special mammogram views to be done in order to better see around the implant.
Recovery & Long Term Outcome
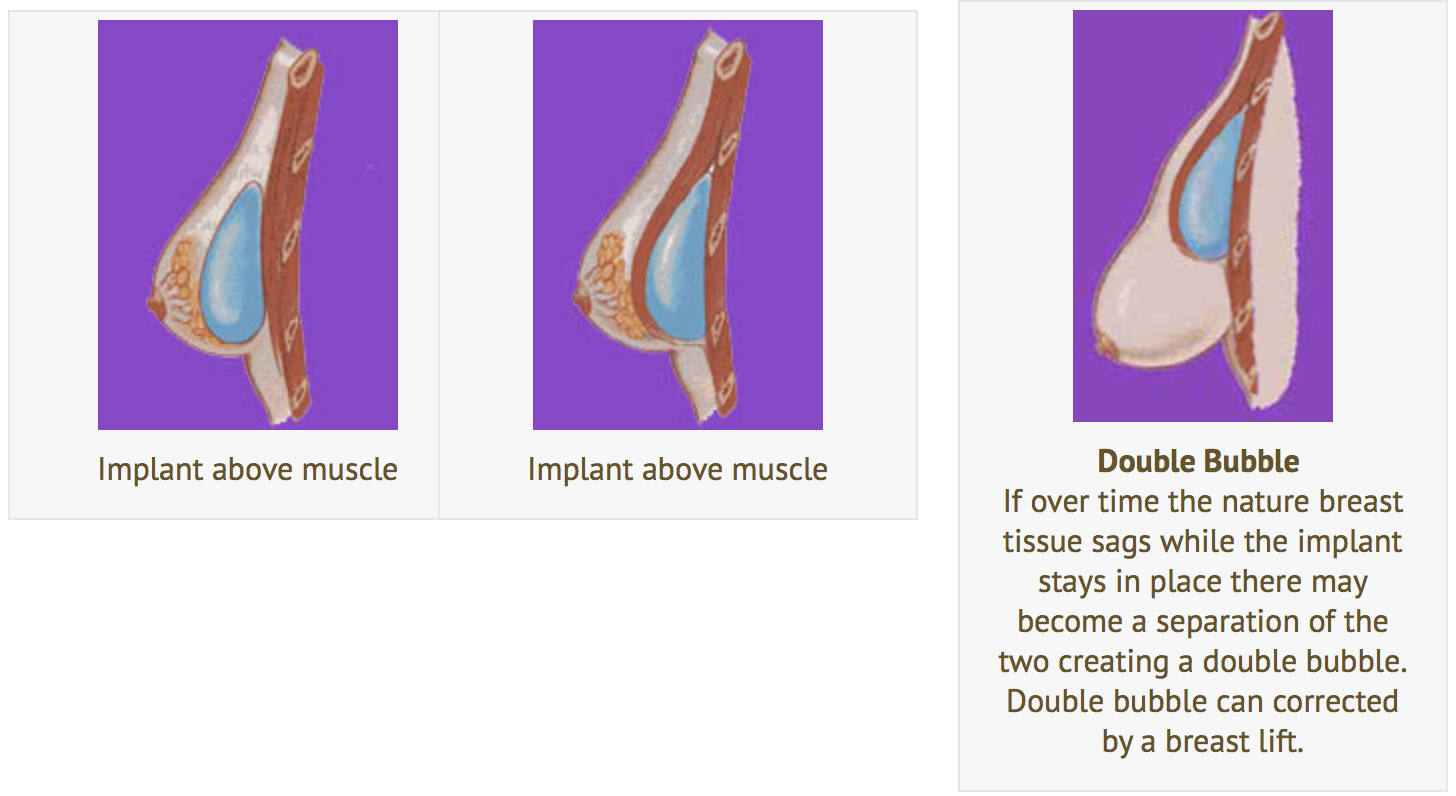
Breast implants are much more resistant to sag than your own breast tissue. If you have little nature breast tissue you will probably never have to worry about sag. If you have a significant amount of breast tissue then this tissue will sag with age just like it would if the implant were not there. If the sag becomes severe you may notice a separation of the implant which stays in place from the nature breast tissue. This is called a "Double Bubble."
This is variable. If you are young and have good quality skin, i.e. no stretch marks, it is likely that your breast will return to your pre-pregnancy state. If you have poor quality skin and/or your natural breast tissue enlarges greatly during pregnancy or breast feeding than some changes will likely result. This usually results in one nipple being slightly lower than the other and/or some degree of sag.
It should be mentioned that these changes would have occurred without the implant. If anything, the immobile volume provided by the implant provides some degree of protection against sag.
There are various scenarios that fall within this category. At the very least, you should discuss this with your plastic surgeon prior to augmentation, so you are fully informed in the event an un-forseen issues arises after surgery.
There is less discomfort if the implant is placed above the muscle. If the implant is placed under the muscle then you can expect the most discomfort for the first 48-72 hours. After this time period, the muscle adapts and the discomfort level drops off quickly. Bigger implants take slightly longer. You will not be able to actively move your shoulders for the first 3 weeks. If you have a sedentary job it is possible to return to work after 3-4 days as long as you do not move your arms too much. In general, you should expect to take a week off work.
If your job requires significant lifting than you will need to take at least 3 weeks off work.
Most plastic surgeons require that you wait at least 6-8 weeks after breast augmentation to begin wearing an under wire bra. This is because the strong support provided by the wire can alter the positioning and/or prevent the "dropping" of the implant into proper position. The reality is you probably will not need an under wire bra because the implants provide more than enough upward support on their own. You will notice that comfortable under wire bras are much harder to buy with implants because the implants are less moldable than your nature breast tissue.
")

